In 2023, Kristin S. Bowman submitted Evaluating the Effect of Physical Prompts on Echoic Responses to Endicott College as part of a Ph.D. in Applied Behavior Analysis. The study focused on autistic children who were not speaking despite intensive behavior therapy. Within this framework, speech was regarded as the preferred modality and a predictor of later independence. The researcher questioned whether adding new techniques could increase speech when standard methods did not work. The experiment examined whether children could be trained to produce speech sounds during ABA therapy.
Bowman described “echoic” sounds as vocal responses repeated by the child that matched what was heard. The intervention in the experiment was designed to measure “success” by the rate of increase in correct responding. The task consisted of the therapist presenting a sound and the child attempting to copy it. The behaviorist used prompts and reinforcement to shape more accurate responses across repeated trials. This, they called therapy, because they found that speech improved with this intervention.

AI picture illustrating a therapist physically guiding a child’s mouth during speech training, highlighting the use of physical prompts in shaping vocal responses.
Participants and Methods
The study was conducted with four children diagnosed with autism spectrum disorder. These children were attending a variety of specialized schools where they received intensive Applied Behavior Analytic (ABA) intervention alongside speech–language and occupational therapies. Participants were selected because they could imitate movement but not speech. Meaning, all children had a demonstrated ability to imitate non-vocal motor actions and/or produced spontaneous vocalizations. Further, participants were recruited only if they showed significant deficits in communication behavior based on standardized assessment in their academic record.
- Sarah (10 years old)
Produced vocal play including humming and approximations of familiar phrases. Communication consisted primarily of requests, often made using a speech-generating device, with some shaped vocal approximations. - Jayden (11 years old)
Produced frequent nonspeech vocalizations, including squeals and reduplicated babbling, with minimal consistent echoic responding. Communication relied on a speech-generating device and gestures. - Benjamin (5 years old)
Demonstrated a limited vocal repertoire with simple sounds and weak imitation. Communication included signs, nonverbal actions, and emerging use of a speech-generating device. - Theo (3 years, 3 months old)
Produced approximations of short utterances and demonstrated broader imitation abilities, though speech remained difficult to understand due to articulation patterns.
For the experiment, each child was taught target sounds across repeated trials. Sessions were conducted in a controlled school environment, with children positioned to allow close physical access for prompting. The arrangement supported repeated trials, precise prompt delivery, and continuous measurement of vocal responding.
In each trial, the therapist presented a sound, and the child was expected to copy it. If the child matched the sound, it was counted as correct and reinforced. If not, the therapist provided more help, sometimes physically guiding the child’s jaw, lips, or mouth to produce the sound. Within this setup, the child heard a sound and repeated it, and that repetition was recorded as “learning”. The study measured whether sounds could be shaped and stabilized during the experiment, not whether verbal behavior relates to authentic communication or expression.
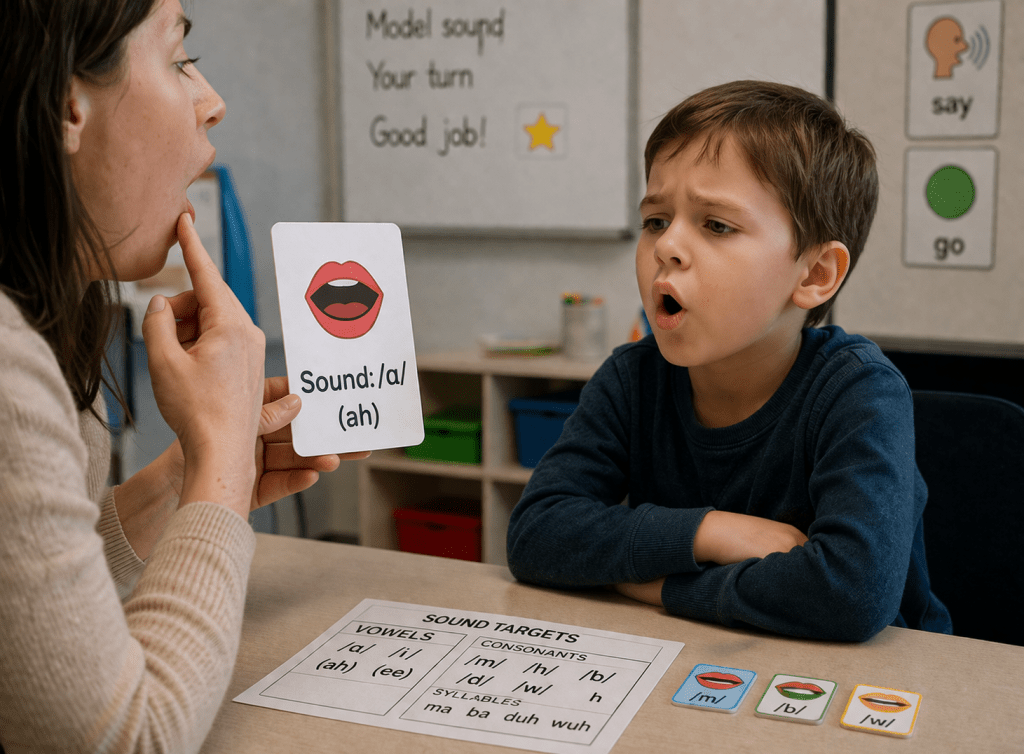
AI image illustrating a behavior technician introducing simple speech sounds (like “ah”) with visual cues, while the child imitates the sound, highlighting sound production compliance as a successful outcome of a behavior intervention.
Physical Support and the Problem of Authorship
The use of physical support in Bowman’s study raises a question that appears in other areas of autism intervention: who is producing the behavior? In signed or typed communication, physical support is treated as a threat to authorship. If a response cannot be shown to originate independently from the individual, it is not accepted by behaviorists as authentic communication. From the behaviorist’s perspective, the verdict is clear; communication must be independently produced to be considered valid.
Here in this study, physical prompting embedded into echoic training also participates directly in producing the response, but it is interpreted differently. The child’s mouth is guided to form a sound, and the result is treated as progress because independence is expected to come later. This creates an asymmetry. The same condition, physically supported behavior, is accepted in one context and rejected in another. What determines the difference is not the presence of support, but whether the outcome matches what the field defines as valid communication. Both involve physical support shaping behavior, but they differ in whether independence is required to count that behavior as communication.
Table showing how both approaches use physical help, but differ in whether the child must be independent for it to count as communication.
| Feature | Echoic Training (Bowman) | Typed Communication / Spelling |
| Type of support | Physical guidance of jaw, lips, and mouth | Physical support of hand/arm or typing device |
| Role of support | Helps produce correct speech sounds | Helps produce typed or spelled responses |
| Independence requirement | Assumed to emerge later (prompt fading) | Required at the time of testing |
| Evaluation standard | Accuracy of sound production | Source control (who authored the message) |
| Prompted responses | Accepted as progress | Considered invalid if not independent |
| Primary concern | Increasing correct vocal output | Verifying validity of expression |
| Interpretation of support | Developmental (step toward speech) | Contaminating (risk of facilitator influence) |
| What counts as communication | Speech-like sounds that match a model | Independently generated messages |
| Underlying assumption | Shaped vocal behavior leads to language | Communication must originate from the individual |
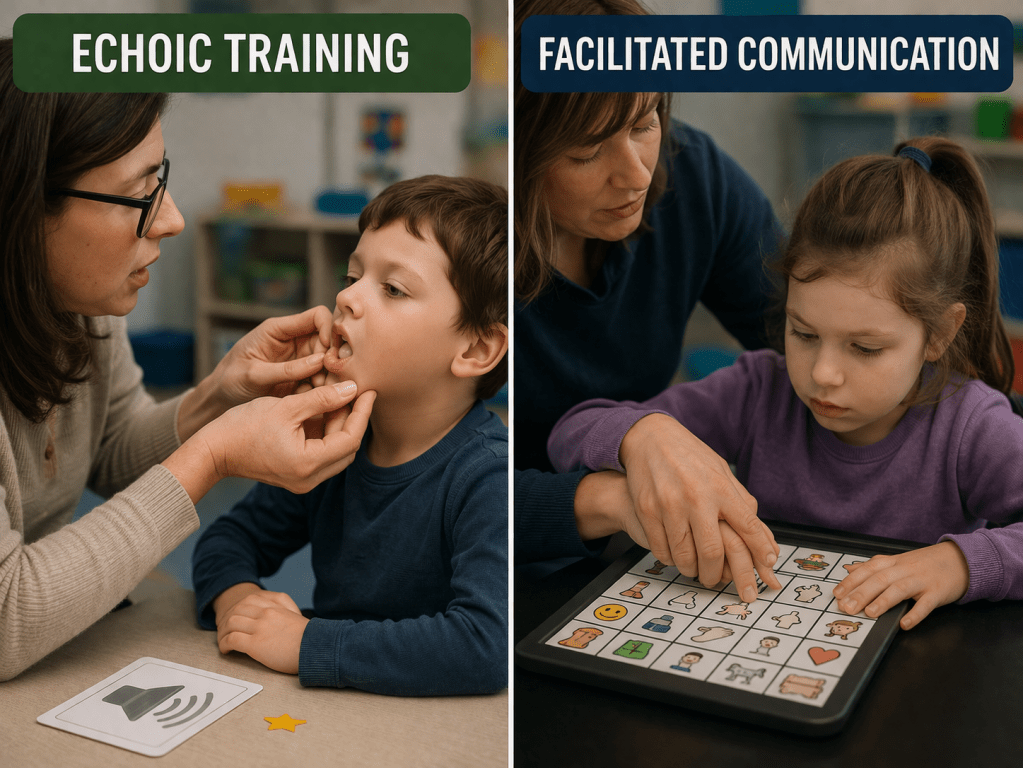
AI image comparing echoic training and facilitated communication, showing how physical support is used in both contexts but interpreted differently as valid or invalid communication.
What Counts as Meaningful Communication
The study measures sound production, not communication. It does not examine whether the child uses these sounds outside the task, initiates them, or uses them to express anything. The study does not report how participant assent or engagement with the task was evaluated. A prompted sound is counted as learning so the system can show progress in their school record. This study was not about helping your child find their voice, but rather proving the intervention is effective on paper.
This is similar to setting a goal for a Deaf child to verbally produce a short “A” sound and then evaluating that sound as a clinical technicality measure. Without context, the sound has no communicative value. It would not be considered a meaningful communication goal in an Individualized Education Program (IEP), nor would it meet standards for medical necessity for health plan reimbursement. When the child is able to reproduce a sound that matches the therapist, it is recorded as an acquisition and interpreted as progress toward language. Meaning, initiation, and social use are not measured in this study.
Repeating a sound when prompted does not show that the child is communicating. It shows that the child can reproduce a sound. Echolalic speech is treated as meaningful because it can be shaped into forms that resemble language. Its value is in how it can be modified, not in what it means for the child. The study treats ‘echoic responding’ as an early form of communication, but this is not shown within the data.
Evaluating speech without meaning is a mere measurement of sound, and does not evaluate communication as it is defined in real-world use. The determining factor is not whether communication occurs, but whether it matches what the system recognizes as valid. This study creates a directional bias. Behavior that resembles speech is accepted as communication. Behavior that does not fit that form is rejected.
These limitations are not isolated to a single study. A five year review of 119 autism intervention studies published in eight ABA journals found widespread undisclosed conflicts of interest among researchers, raising concerns about scientific integrity and oversight. Of 450 authors, 78% had clinical or consulting ties, and 93% of papers included at least one author with such a conflict, yet only 8% disclosed any conflicts. Most “no conflict” statements were inaccurate, leading the authors to conclude that this level of non-disclosure reflects a systemic neglect of transparency standards in ABA research and highlights the need for stronger accountability in reporting practices.
Scope Expansion: When Behaviorists Become Speech Therapists
Speech is one form of communication, not its definition. People communicate using speech, gestures, writing, devices, and other modalities. The goal of intervention is not the production of a specific form, but the effectiveness of communication.
Speech–language therapy is a specialized field focused on clarity, function, and use of communication. In this study, speech-shaping procedures are used, but outcomes are evaluated as performance within a task rather than communicative function. The study shows that sounds can be produced under structured conditions. It does not show that these sounds improve communication for the individual.
The procedures described in the study overextend the reach of behaviorism. The intervention functions as “scope creep”, associated with speech–language pathology, where professional training involves specialized knowledge of phonology, motor speech disorders, and communication development. In practice, these services are often delivered by minimally trained staff, including high school graduates, operating under limited supervision. This creates conditions where neglect can occur, as children receive intensive intervention without the level of expertise, oversight, or accountability expected in comparable clinical fields. Appropriate supervision is necessary to prove that services were rendered or else it constitutes federal fraud.
The data in this study show increases in accuracy under prompting, but do not demonstrate that the skill is learned, retained, or used without assistance. A speech therapist can adequately assess the fact that if the child needs physical help again and again, they are not doing it on their own.
From an instructional design perspective, an effective teaching model must show not only acquisition within the task, but durability, generalization, and independence. These outcomes are not established in the study. The procedure produces correct responses under controlled conditions, but does not show that those responses persist or transfer beyond the training context.
Within the study, these procedures are framed as behavior analytic intervention, without addressing the distinction between disciplines. Techniques associated with speech–language pathology are used to shape articulatory movement, while outcomes are interpreted as behavioral acquisition. This creates a form of scope expansion, where methods from one field are incorporated into another without adopting its standards for training, evaluation, or outcome measurement.
What Parents Should Ask
If your child is receiving therapy, it is important to understand what is being measured and what is being promised. Producing sounds during therapy is not the same as communicating. Ask whether your child is using those sounds independently, in real situations, to express wants, needs, or thoughts. Communication is defined by use, not just by form.
Speech is one way to communicate, but it is not the only way. Many children communicate effectively using gestures, devices, or other methods. The goal of intervention should be meaningful communication, not just sound production.
If therapy includes goals related to speech or communication, you can ask:
- Who is trained to provide this type of intervention?
- How is communication being measured outside of structured sessions?
- Does the skill generalize to everyday situations?
Understanding these distinctions helps ensure that the focus remains on your child’s ability to communicate, not just their ability to produce sounds during practice.
If you are being promised “communication” goals within behavior-based treatment, it is important to understand what is being delivered and who is qualified to provide it. Speech and language intervention is a specialized field, and not all providers are trained or licensed in this area. When treatment moves across disciplines, it raises important questions about scope of practice, leading to “scope creep”. This raises concerns about scope of practice and whether services are being delivered within appropriate professional boundaries. Clarifying these points helps ensure that services remain appropriate, transparent, and focused on meaningful communication.
These concerns extend beyond research and into policy. Testimony was submitted to the Senate Health Committee by the Doogri Institute presenting audit findings and raising questions about the structure and outcomes of ABA services. The focus expanded from administrative oversight to how the system operates and what it produces. These issues are now formally part of the legislative record and within the scope of state-level consideration.
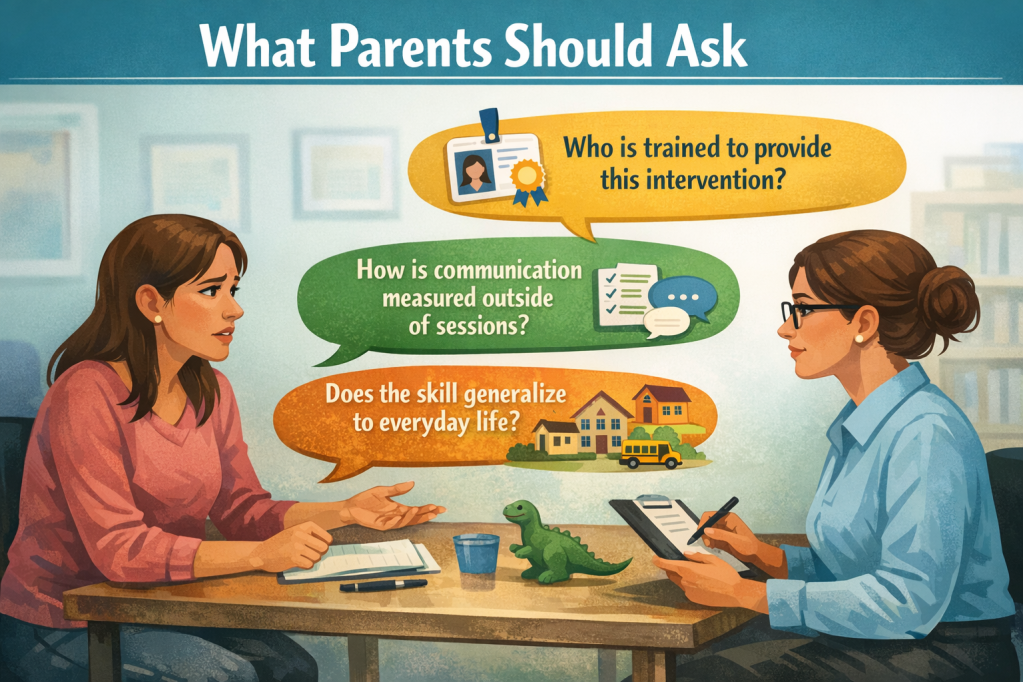
AI illustration of a parent asking critical questions about therapy goals, measurement, and whether skills truly carry over into real-life communication.
Scope Expansion and the Promise of Speech
The study demonstrated that physical prompting increased the likelihood of producing specific vocal targets under controlled conditions. From this, a broader implication was drawn that these procedures contributed to the development of functional speech. This claim extended beyond the data. This pattern is not limited to research claims, but is reflected in how the industry responds to scrutiny, often reframing practices without changing the underlying model (see: Dosing as Damage Control).
The findings in this study showed that prompted responding could produce correct sounds within a structured task. They did not establish that these sounds generalized beyond the participants, the setting, or the conditions of prompting. Generalization, independence, and functional use were not measured. Without these, the results remained limited to performance within the task.
The study does not evaluate whether these sounds were used independently, across contexts, or in social interaction. It does not assess spontaneous communication in real life. The link between prompted sound production and meaningful communication was assumed, not demonstrated.
For families, this assumption carries practical consequences. Framing echoic gains as communication suggests a pathway toward speech and independence. The study showed that sounds can be produced during structured practice. It does not show that this leads to independent, functional communication.
The Boundary of Behavioral Authority
The comparison with facilitated communication clarifies the boundary conditions of what is recognized as communication within behavior analysis. Prompted vocal behavior is accepted because it is structured to become independent and conforms to expected speech forms. Supported communication is rejected when independence cannot be demonstrated, even if it functions communicatively for the individual. Both cases involve physical support influencing behavior. They diverge on what counts as valid evidence.
Behavior analysis requires independence to attribute communication. At the same time, it accepts prompted production as progress when it aligns with its instructional model. This creates a system in which certain forms of supported behavior are legitimized while others are excluded.
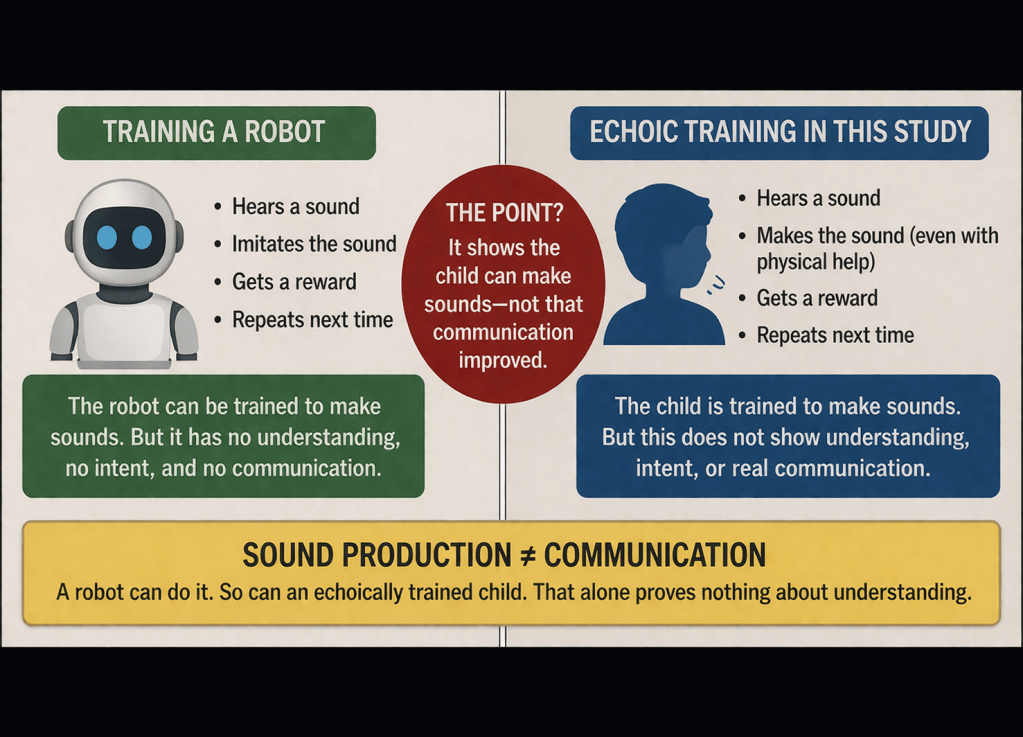
Bowman’s study operates within this boundary. Its findings are valid within its design. Physical prompts increase correct responding. The procedure produces speech-like output. The study shows that vocal forms can be shaped. It does not show that those forms function as communication. It shows how to train sounds, but not how children come to communicate.
So I can train a robot. What is the point of training the robot to make sounds? It doesn’t show improvement of anything-it shows the child can make sounds.

Leave a comment